Governance Working Group

The Governance Working Group was established as part of the ANHP OHT framework. Its responsibilities include:
Develop structures and processes – Recommend how the larger partnership or organization should be organized (committees, councils, reporting lines, terms of reference).
Clarify roles and responsibilities – Define who has decision-making authority, and how accountability is maintained.
Create or review policies – Draft governance policies (conflict of interest, membership, leadership selection, meeting procedures, etc.).
Ensure compliance – Make sure governance aligns with laws, regulations, and agreements.
Promote transparency – Establish how information and decisions will be shared with members and stakeholders.
Support equity and inclusion – Ensure that diverse voices, especially from key stakeholders or community partners, are represented in governance.
Evaluate effectiveness – Regularly review whether the governance model is working and recommend changes if needed.
BACKGROUND:
In the Spring of 2015, the critical shortage of physicians serving the Kenora area was addressed in a deputation to Kenora City Council entitled Kenora Health Care – A Growing Industry Sector: The Importance of Physician Recruitment and Retention, Community Vision and Collaboration (A Physician Perspective). The presentation focused on five key areas:
- The importance of physician recruitment and retention, and the need for a centralized physician recruitment process for the Kenora area;
- The current state of health care in the Kenora area;
- An update on changes to health care affecting the Kenora area;
- A proposal for a community-based Health Care Commission; and
- The role of the City of Kenora in moving these issues forward.
In response, the City spearheaded the creation of the Kenora Area Health Care Working Group in September 2015. At that time, the group included representatives from the City of Kenora, Lake of the Woods Development Commission, Lake of the Woods District Hospital, Waasegiizhig Nanaandawe’iyewigamig, Kenora Chiefs’ Advisory, Northwestern Health Unit, family physicians, and members of the community. The working group identified three key issues: (1) physician recruitment and retention; (2) cross border access to care between Ontario and Manitoba; and (3) the need for a long-term collective vision for health care in the Kenora area.
In less than a year, the working group completed a needs assessment, raised funds from committed stakeholders, and hired a healthcare professional recruiter. In less than two years, the working group made progress on the cross-border issue, identified the replacement of aging hospital infrastructure as an additional key priority in support of both successful patient care and physician recruitment, and secured funding begin a formal planning process.
Political leadership comprised of Grand Council Treaty#3 Ogichidaa, the Mayors of the City of Kenora and the Township of Sioux Narrows/Nestor Falls, Chief Lorraine Cobiness on behalf of the Kenora Area First Nation Chiefs, and the President of the Kenora Métis Council assembled in the roundhouse at Wauzhushk Onigum First Nation to sign a resolution agreeing to work together in partnership to develop an All Nations health care system, including construction of an All Nations hospital and campus, with the express purpose of improving health outcomes for all people of the region it serves through a healthcare service model built on a partnership between First Nations, Métis, and non-First Nations governments and providing an improved healthcare system that reflects the specific needs and costs of the north.
The signatories to this document now wish to work together to grow and evolve the working group to create the All Nations Health Partners, a coalition of leaders in Indigenous and mainstream health services in the Kenora Region, and of other stakeholders, through this collaborative decision-making framework agreement.
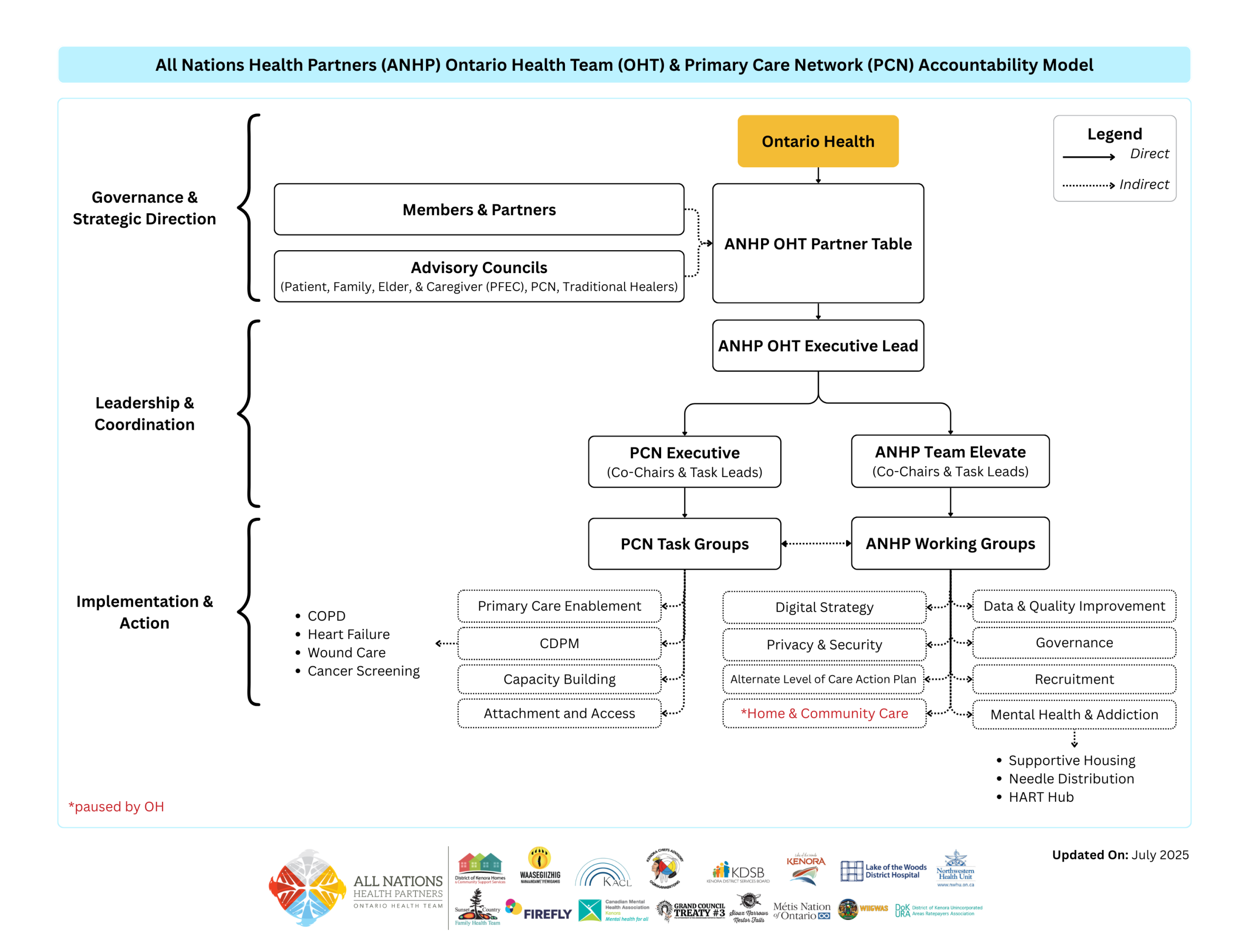
A pictorial of the initial All Nations Health Partners model is set out below:
The Team Members agree as follows:
- Definitions. Capitalized terms used in this Framework have the meanings given to them in Schedule 1.
- February 16, 2017 Resolution. The February 16, 2017 resolution, which gave rise to the ANHP, formed in ceremony and trust, is attached as Schedule 2.
- Team Members. The current Team Members are listed in Schedule 3. Additional organizations may be admitted as new Team Members through a process established by the ANHP Council provided that they become a signatory to this Framework.
- Framework. This Framework sets out the purpose, function, and processes for the ANHP. It is a living document, and will evolve over time. At any time, a Team Member may propose changes to this Framework for discussion at an ANHP Council meeting. Changes will only become effective upon approval by the ANHP Council.
- Shared Objective. The Team Members will work together to facilitate the development and implementation of the Shared Objective, and will be guided by the Truth and Reconciliation Commission’s Health Calls to Action Nos. 18-24.
- Seven Sacred Teachings. The ANHP will work by consensus and will be governed by a culture of ethical conduct embodied in the Seven Sacred Teachings:
VALUE APPLICATION IN CONTEXT Honesty Speak openly and truthfully always. Truth Focus on facts; be prepared to accept information you may not want to hear. Respect Everyone has value, and should be treated with respect. Being on time, listening, and speaking humbly, and respecting personal boundaries are all ways in which respect is demonstrated. Bravery Take risks; move toward your vision despite fears and unknowns. Have the courage to engage in sensitive or difficult conversations. Love Love describes the good life – minobimaadiziwin. It is given and received through life, earth, people, choices and opinions. Humility No one person or community is more important than another; we are all equal. Everyone has a voice, and all contributions have value. We all have gifts as well as limitations. Wisdom We constantly learn by listening, hearing, and applying what we learn – especially from our elders – in a never-ending process. - Purpose of this Framework. The purpose of this Framework is to:
- set out how the Team Members will work together to achieve the Shared Objective;
- establish the ANHP Council, PFEAC, THAC, PSAC, and other organizational structures to enable the work of the Team Members; and
- set out the rights and obligations of the Team Members.
- Commitments. The Team Members confirm their commitment to:
- participate in the collaborative decision-making structures and processes described in this Framework to achieve the Shared Objective;
- embody the Seven Sacred Teachings in their work;
- try to eliminate, minimize, or mitigate any conflict between the Shared Objective and any of their own contractual and service obligations and relationships; and
- adhere to the provisions of this Framework.
- Autonomy/Non-Derogation. While the Team Members have a Shared Objective, each Team Member remains autonomous, and is responsible to its own governing body. The ANHP Council has no authority to make a decision binding on an individual Team Member, except as specifically set out in this Framework or as specifically delegated by a Team Member through a Project Agreement or otherwise.
- ANHP Council. The Team Members establish the ANHP Council as the collaborative decision-making body of the ANHP, and for the implementation of ANHP and ANHP-OHT initiatives in pursuit of the Shared Objective. The ANHP-OHT is part of the work of the ANHP, and the ANHP Council will oversee the work of the ANHP-OHT. The composition, mandate, and processes of the ANHP Council are set out in Schedule 10.
- ANHP-OHT. As part of the Shared Objective, the Team Members, through the ANHP, intend to be designated by the Minister of Health as an Ontario Health Team under the Connecting Care Act, 2019 and, once designated, to operate under the name All Nations Health Partners ‒ Ontario Health Team.
- ANHP-OHT Goals. The ANHP-OHT’s goals include:
- improved health care services for everyone;
- responsiveness to the needs of Indigenous communities;
- seamless continuum of care across all healthcare providers;
- access to health services closer to home;
- health outcomes that exceed Provincial standards;
- supportive environments for healthcare providers; and
- building an All Nations hospital and campus.
- Community Role and Engagement. The ANHP Council will engage the community in system co-design and in all levels of ANHP-OHT decision-making to ensure that the voice of those who seek or receive care or services from the ANHP-OHT, or who support those seeking or receiving care or services, is heard. The Team Members, through the ANHP Council, will establish a Patients, Families, and Elders Advisory Council (“PFEAC”) with terms of reference substantially similar to the draft terms of reference set out in Schedule 13. Representation from the PFEAC will be included in the ANHP Council as provided in its Terms of Reference and in the committees and working groups of the ANHP Council as appropriate. A Patient Declaration of Values for the ANHP will be established by the ANHP Council in consultation with the PFEAC.
- Traditional Healers Advisory Council. The ANHP Council will engage traditional healers in system co-design and in all levels of ANHP-OHT decision-making to ensure that the voice of those who provide care or services through the ANHP-OHT is heard. The ANHP Council will support the establishment of a Traditional Healers Advisory Council (“THAC”). Representation from the THAC will be included in the ANHP Council as provided in its Terms of Reference and in the committees and working groups of the ANHP Council as appropriate.
- Primary Care and Specialist Care Role and Engagement. The ANHP Council will engage primary care and specialist providers in system co-design and in all levels of ANHP-OHT decision-making to ensure that the voice of those who provide care or services through the ANHP-OHT is heard. The ANHP Council will support the establishment of a Primary Care and Specialist Care Advisory Council (“PSAC”). Representation from the PSEAC will be included in the ANHP Council as provided in its Terms of Reference and in the committees and working groups of the ANHP Council as appropriate.
- Communication and Engagement. The ANHP Council will develop and implement a central communication and engagement strategy intended to actively engage all interested stakeholders, and to keep Team Members, residents, and other key stakeholders informed about the ANHP’s progress. The strategy will include a plan describing distribution and alignment of key messages, target audiences, and communication type and frequency. For ANHP-OHT matters, the ANHP Council is collectively responsible for seeking input from and relaying information to all Team Members. Special attention will be paid to have communication protocols in place to connect all primary care providers in the ANHP OHT with other ANHP OHT members and partners.
- ANHP-OHT Projects. To fulfill the Shared Objective, the Team Members will carry out Projects. Each Project will be implemented in accordance with Schedule 17.
- Information Sharing, Transparency, Privacy and Confidentiality. Transparency will be a key enabler for fulfilling the Shared Objective. Each Team Member will communicate decisions or positions taken by its organization that impact the work of the ANHP in a timely and transparent manner. The Team Members will adhere to the provisions for information sharing, transparency, privacy, and confidentiality set out in Schedule 18.
- Voluntary Integration with Others. If a Team Member is contemplating an integration with another entity or entities that will have a significant impact on the Shared Objective, then it will notify the ANHP Council, and the other Team Members in writing at least 90 days before the completion of such integration. The notice will describe: (a) name of the entity or entities; (b) terms of the proposed integration; and (c) assessment of the impact, if any, of the proposed integration on the ANHP and the Shared Objective. Within 21 days of receipt of the notice, the ANHP Council will assess the impact of the proposed integration on the ANHP and deliver a written report with recommendations to the Team Members. If any Team Member objects to the proposed integration, it will deliver a notice advising the ANHP Council of its objection within 21 days of receipt of the report and the matter will be submitted to the dispute resolution provisions set out in Schedule 21.
- Involuntary Integration with Others. The Team Members recognize that the Minister of Health may order an integration between one or more of the Team Members and/or one or more third parties. If this occurs, the ANHP Council will meet and develop a recommendation to the Team Members as to the impact of such integration on this Framework, the ANHP, the ANHP-OHT, and each Project, and whether any amendments are required to this Framework, a Project, or a Project Agreement. The Team Members will try to continue this Framework and each Project unless any Team Member determines it is not feasible to do so where the essential benefits of this Framework or a Project will not be realized by the ANHP. If any Team Member makes this determination and any other Team Member does not agree, the matter will be submitted to the dispute resolution provisions set out in Schedule 21.
- Dispute Resolution. The Team Members will use their best efforts to avoid disputes by clearly articulating expectations, establishing clear lines of communication, respecting each Team Member’s interests, and respecting the Seven Sacred Teachings. However, if a dispute arises, the Team Members will follow procedures set out in Schedule 21, acting in good faith.
- Term. This Framework will start on the Effective Date and will continue indefinitely, unless terminated by the mutual written agreement of all Team Members.
- Voluntary Withdrawal. A Team Member may withdraw from this Framework by providing at least 90 days’ notice to the other Team Members and to the ANHP Council.
- Expulsion. A Team Member may be expelled from the ANHP, and thereby cease to be a party to this Framework. Reasons for expulsion may include if the Team Member is not meeting its commitments under this Framework, a Project, or a Project Agreement, is no longer committed to the Shared Objective, or is disruptive to the consensual decision-making process at the ANHP Council, or any of its committees or working groups. An expulsion will only take place after following the procedures set out in Schedule 24.
- Withdrawals/Termination of Project Agreement. Unless a Project Agreement provides otherwise: (a) the parties to a Project Agreement may terminate the Project Agreement by mutual written agreement, provided that they give at least 90 days’ notice to the ANHP Council; and (b) a party to a Project Agreement may withdraw from the Project Agreement by giving at least 90 days’ notice to the ANHP Council and the other parties to the Project Agreement.
- Consequences of Termination, Withdrawal or Expulsion. A Team Member that withdraws or is expelled from this Framework will cease to be a party to this Framework. Termination of, or withdrawal or expulsion from, this Framework will not automatically constitute termination of, or withdrawal or expulsion from, any Project or Project Agreement. Withdrawal from or termination of one Project or Project Agreement will not automatically constitute withdrawal from or termination of this Framework or any other Project or Project Agreement. A Team Member that terminates, withdraws from, or is expelled from a Project, a Project Agreement, or this Framework will remain accountable for its obligations, and its actions and omissions before the effective date of the withdrawal or expulsion, and will work with the ANHP Council to develop strategies to reasonably fill any resource or service gaps left by the termination, withdrawal, or expulsion.
- General Provisions. General contract provisions that govern this Framework are set out in Schedule 27.
- Signature Pages. The signature pages for the Team Members are attached as Schedule 28.